Sticking Points - Reducing Excess Fingerstick Blood Glucose Testing In Hospitalized Patients With Well-Controlled Type 2 Diabetes Mellitus: A Quality Improvement Project
Samir Kamat BA1, Jared Dashevsky, M.E.1, Alyssa Gontzes, MS1, Madeline Floodstrand, MS1, Grenye O’Malley, MD,1,2 , Anne S. Linker, MD1,3
-
Icahn School of Medicine at Mount Sinai
-
Division of Endocrinology, Diabetes, and Bone Diseases, Icahn School of Medicine at Mount Sinai
-
Division of Hospital Medicine, Mount Sinai Hospital
1. Specific Aims of the Project
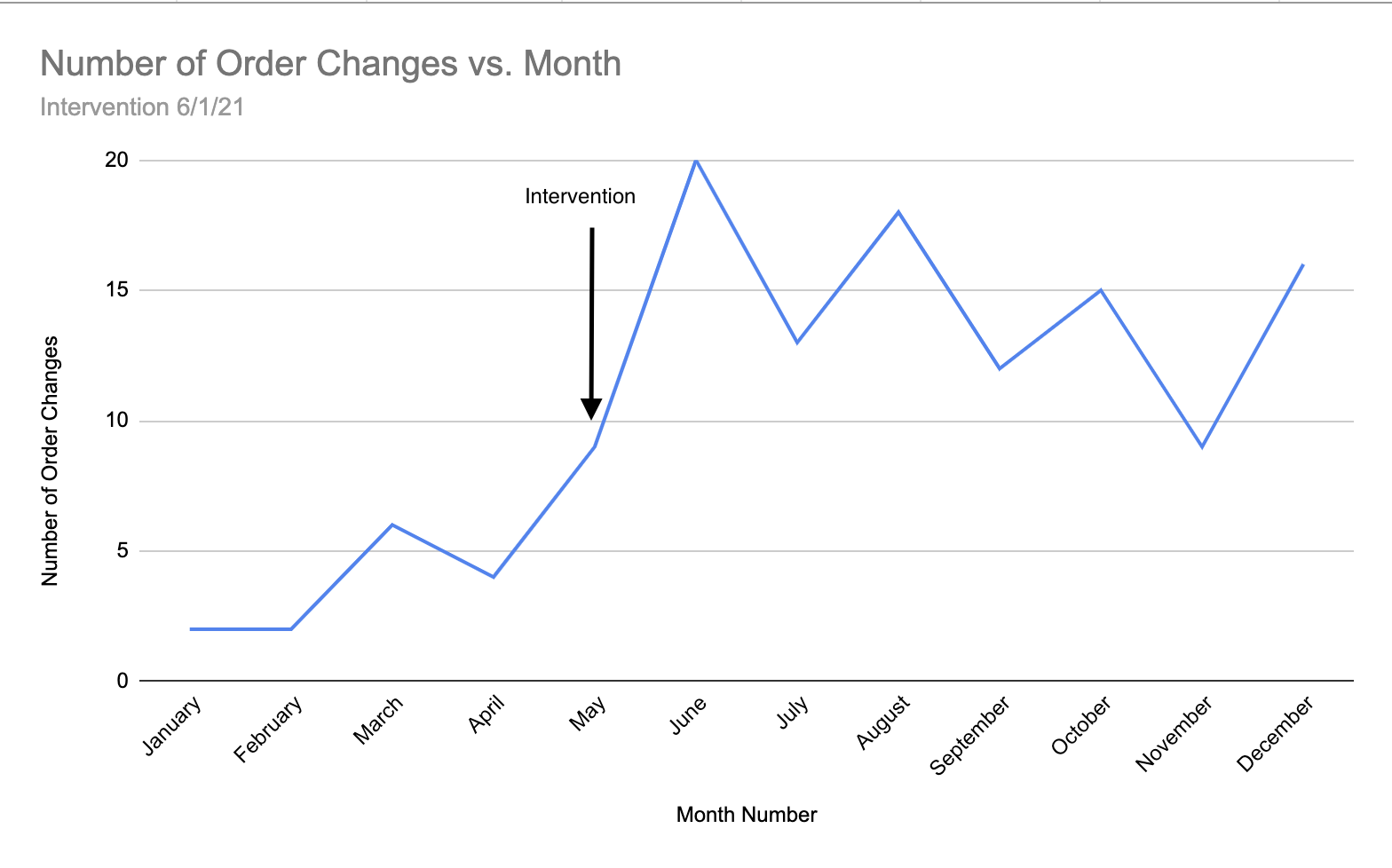
Outcome measures included the number of FSBG order changes per month, the percentage of low-risk patients with T2DM receiving BID FSBG or who had the FSBG order discontinued, and the total number of fingersticks avoided. We defined an "order change" as a QID to BID order change or a canceled QID or BID order. Our post-intervention analysis found a significant 208% relative increase in the number of order changes per month, from 4.60 orders to 14.71 orders (p<0.01). The percentage of qualifying patients whose FSBG order changed increased 115% during the post-intervention period from 2.90% to 4.93%, avoiding 1,541 fingersticks and saving $14,000 in costs related to supplies and nursing time.
3. Significance of Results
Our findings suggest the EMR and educational interventions are feasible, despite only affecting a small population thus far. The intervention can be scaled to make a more significant impact on the avoidance of excessive FSBG testing in low-risk patients with T2DM at our institution.
Avoiding excessive FSBG testing not only optimized patient care but also improved nursing workflows and reduced healthcare costs. Our preliminary nurse perception survey found that nurses spent on average 5 minutes administering one FSBG test, a process estimated to cost $9. Therefore, the 1,541 fingersticks avoided saved over five days of nurses’ time and $14,000. Nurses, theoretically, had more time to focus on caring for other patients or tasks. Though the project impacted workflows, there were missed opportunities and limitations despite our educational campaign. Our project occurred concurrently with two surges of Covid-19, during which most educational sessions occurred remotely. We believe this reduced the impact of our educational interventions, as it was more challenging to make providers aware of the available FSBG order modification, and this intervention became a lower priority for front-line providers. However, we saw an initial uptick in order changes when the EMR order set was updated before our educational intervention began. This suggests that the EMR order set intervention was critical to affecting change in the context of limited education given Covid-19 restrictions. In a setting without the challenges of Covid-19, we believe the efficacy of our intervention would have significantly improved, resulting in more FSBG tests avoided and time and cost savings.
Overall, these results suggest we improved the value of care delivered to patients by (1) avoiding patient discomfort through excessive FSBG testing and (2) minimizing low-value waste of resources.
4. Lessons Learned:
We gained a firsthand immersion in the quality improvement process throughout the entire process. We now recognize the number of key stakeholders and the iterative process required to implement even a small change. For example, we accomplished managing various components and stakeholders by delegating responsibility to individual team members, such as remote education, troubleshooting EMR issues, or tracking patient safety information. We also appreciate having champions and mentors who helped grease the wheels whenever we experienced setbacks. For example, having our physician mentors accompany us on our educational outreach helped provide legitimacy from the perspective of frontline staff. This project has given us a deep belief in our ability to enact change and improve patient safety through quality improvement efforts.
5. Plans for Future Work
We hope to scale our project to have an even more profound impact across the Mount Sinai Health System. This may involve identifying other opportunities for continued education around the quality improvement effort, expanding the intervention to include non-medicine floors, and raising awareness of our findings to clinicians at different hospital sites.
Acknowledgments:
We are grateful to the Society of Hospital Medicine for providing grant funding, allowing us to pursue this pilot project. We are also thankful for the EMR staff, nurses, residents, and others who helped make this project possible.
|
Order Changes |
Pre_Intervention |
CI (95%) |
Post_Intervention |
CI (95%) |
% Change |
|
Total Number of Low-Risk Patients with Order Changes |
23 |
71 |
208.70% |
||
|
Number of Order Changes/Month (SD) |
4.600(2.966) |
[3.437,5.763] |
14.71(3.729) |
[13.67, 15.76] |
219.88% |
|
Outcome Measures |
Pre_Intervention |
Post_Intervention |
% Change |
||
|
Total fingersticks administered among pts who meet criteria |
20,199 |
27,168 |
|||
|
Percent of patients with Type 2 DM receiving FSBG twice per day instead of four times per day |
0.80% |
2.29% |
|||
|
Percent of patients with Type 2 DM receiving FSBG twice per day or no times per day instead of four times per day |
2.29% |
4.93% |
|||
|
Total Fingersticks Saved |
412 |
1541 |
274.03% |
||
|
Total costs saved |
$3,708.78 |
$13,867.99 |
273.92% |
||
|
Total Nursing Time Saved |
1 days 10:20:25 |
5 days 08:24:26 |
Bloggers




























































