Assessing Influence of Different Educational Strategies on Resident Lab Ordering Behavior: A Prospective Cohort Study
Project Mentor: Dr. Caleb Murphy, Section of Hospital Medicine, University of Chicago
Site Mentor: Dr. Sandhya Wahi-Gururaj, Professor of Internal Medicine, Kirk Kerkorian School of Medicine at University of Nevada - Las Vegas
1. Project Aims
High-value care, which prioritizes healthcare interventions that provide the best patient outcomes at the lowest cost, is an important concept in modern medicine and is especially applicable in the context of laboratory test utilization. Ensuring that labs are ordered only when necessary has the potential for widespread benefits, from minimizing discomfort and iatrogenic anemia from excessive phlebotomy, to improving efficiency in triaging of labs for patients in time-sensitive scenarios, to reducing costs incurred by hospitals and patients. Frequency of lab ordering is often dependent on provider preference; given the lack of standardized protocol in this area, some labs, such as complete blood count (CBC) and serum electrolyte panels (SEP) may be ordered on a daily basis, even in otherwise stable patients, unless providers make a conscious effort towards ordering only as necessary.
Educating providers on this topic is an excellent first step towards improving the practice of ordering labs only as needed. To that end, our study aimed to test the efficacy of different educational strategies on lab utilization of internal medicine residents at our medical school’s primary teaching hospital, University Medical Center of Southern Nevada.
2. Intervention and Preliminary Results
Our intervention took place over a 6-month period. We started by providing a common level of high-value care awareness to residents in the program, followed by allocating teaching services to three arms that involved different educational prompting strategies.
We began with a one-time high-value care conference at resident noon didactics to cover basic principles of inpatient high value care. This was delivered to most residents live at this didactics session, and all residents in the program were also emailed this content for review. Additionally, simple informational posters were placed in resident workrooms that asked the reader if their patients needed daily labs and to rethink ordering repetitive CBC and SEP labs in stable patients (Figure 1).

Figure 1: Informational posters placed in physician workrooms as part of background high-value care education for residents in all arms.
For the intervention, our internal medicine residency program’s three inpatient teaching services were randomized to one of three intervention arms, in which residents were to receive one of two prompts or no prompt at all. Prompts were drafted by Dr Murphy and the student lead and revised through iterative team review. Prompts were also analyzed using Grammarly language editing software to ensure similar language complexity. Prompts were delivered to residents through two means: a WhatsApp message sent during the first and third week of a four-week rotation and verbal reminders from attending physicians at the beginning of each week.
One team was assigned to receive “Education-Oriented” prompts. This group received reminders of the harms of wasteful lab utilization, but without any specific guidance to order labs appropriately. Another team was assigned to receive “Action-Oriented” prompts. This group received regular nudges to review labs weekly and order labs at a less-than-daily frequency in stable patients. The third teaching service received no prompts or education, other than the initial high-value care conference and informational posters, thus representing a control group to compare against the other two arms. The two prompt-based interventions are summarized in Figure 2.
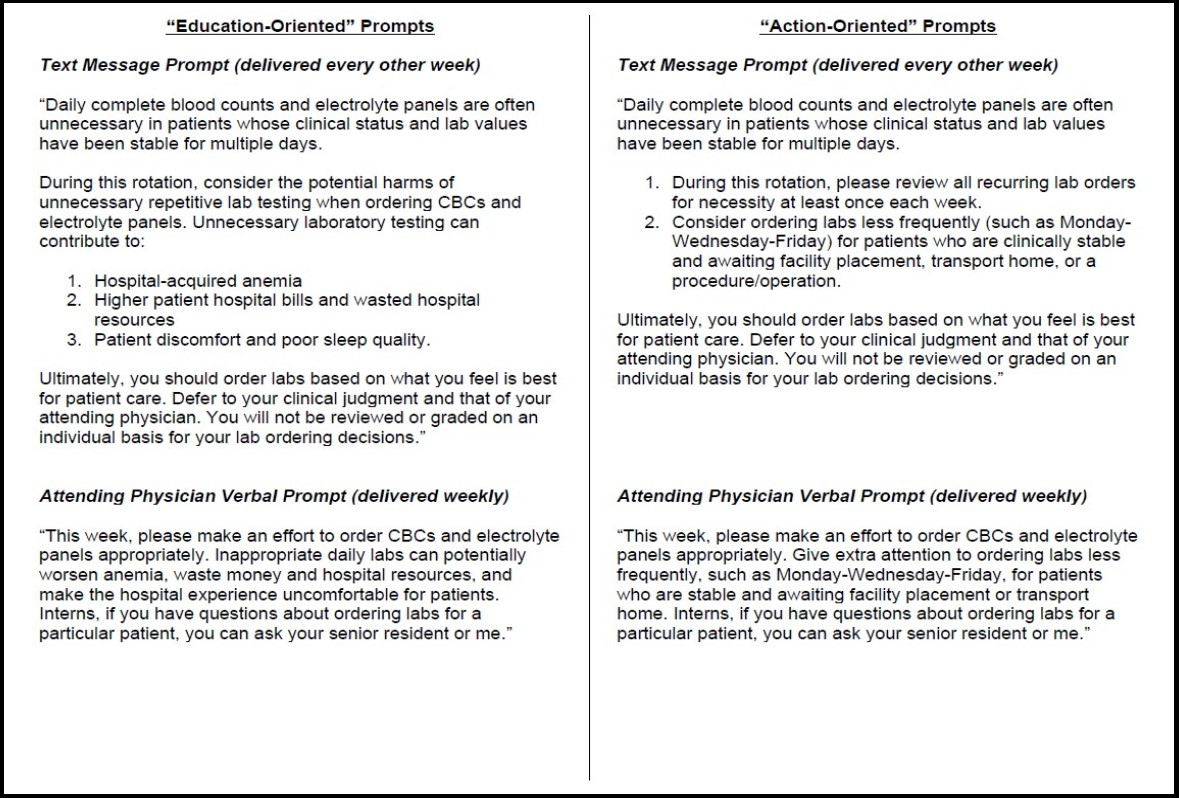
Figure 2: Prompting protocols of “Education Oriented” group and “Action Oriented” group
3. Preliminary Results and Significance
The primary outcome of interest was daily labs ordered per patient day per encounter, with “daily labs” defined as the sum of complete blood counts, basic metabolic panels, renal function panels, and comprehensive metabolic panels. In the pre-intervention and intervention periods, the teaching service receiving Education-Oriented prompts ordered 2.10 and 2.19 labs/day (p=0.21), the teaching service receiving Action-Oriented prompts ordered 2.11 and 1.98 labs/day (p=0.093), and the control service ordered 2.04 and 2.14 labs/d (p=0.19), respectively. Patient characteristics and resident switches between teams were similar between intervention arms in the pre-intervention and intervention periods (see Table 1).
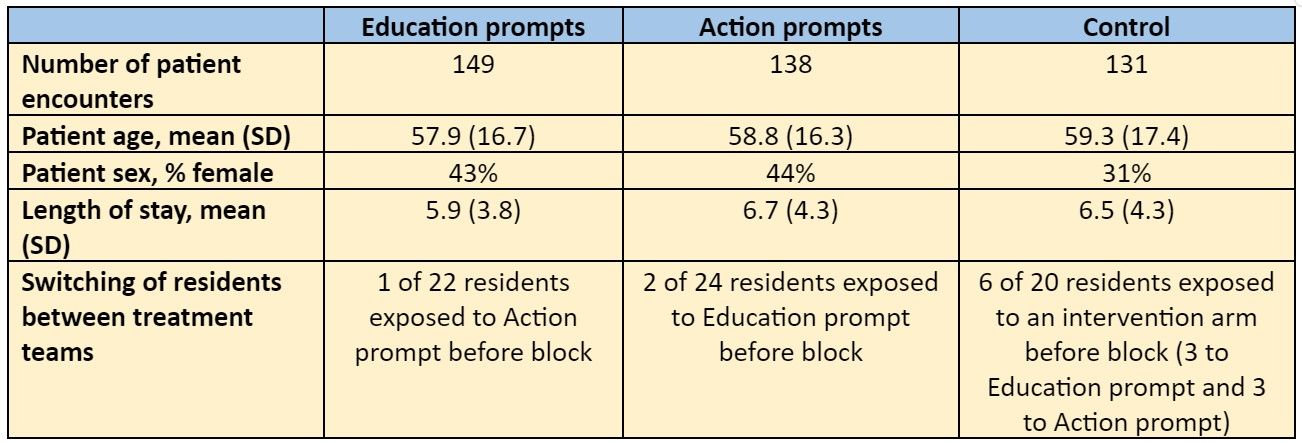
Table 1: Intervention period encounter characteristics
In our preliminary analysis, no statistically significant pre-post change in lab utilization was noted among medicine teaching services who received Education- or Action-Oriented prompts encouraging appropriate lab utilization. However, the Action-Oriented prompt team saw a modest decline in lab orders that approached statistical significance.
4. Lessons Learned and Future Directions
Our intervention failed to show a statistically significant decrease in lab utilization with either prompting strategy. However, the aforementioned decrease in lab orders in the action-oriented prompt group is encouraging and may indicate potential of this intervention to produce significant results in the future with further adjustments, which could have implications for the design of high value care curricula and educational materials. Of course, any conclusions drawn from the final statistical analysis will be limited by our study’s single-site nature. Difficult external circumstances in the community led to the intervention being paused for 1 month of the study period, which led to a further reduction in data collection. Lastly, as noted in Table 1, there is some unavoidable crossover where some residents were exposed to more than one arm of the study, which complicates intervention impact attribution.
While this preliminary analysis has provided valuable insights into the intervention as a whole, there is more work to be done before the full data set is completely analyzed. Next steps are to complete data cleaning and statistical analysis, including controlling for patient and physician characteristics, which may or may not affect statistical significance of the current results. In terms of future directions, replicating this study across a larger time-span and over multiple sites would also more accurately capture any potential effects of the different prompting strategies. Automation of the reminder system, rather than relying on the study team, would improve efficiency of this study design. Lastly, as education-only interventions may be limited in nature, exploring alternative interventions such as decision-making tools or automatic prompts could yield useful insights.
Bloggers




























































